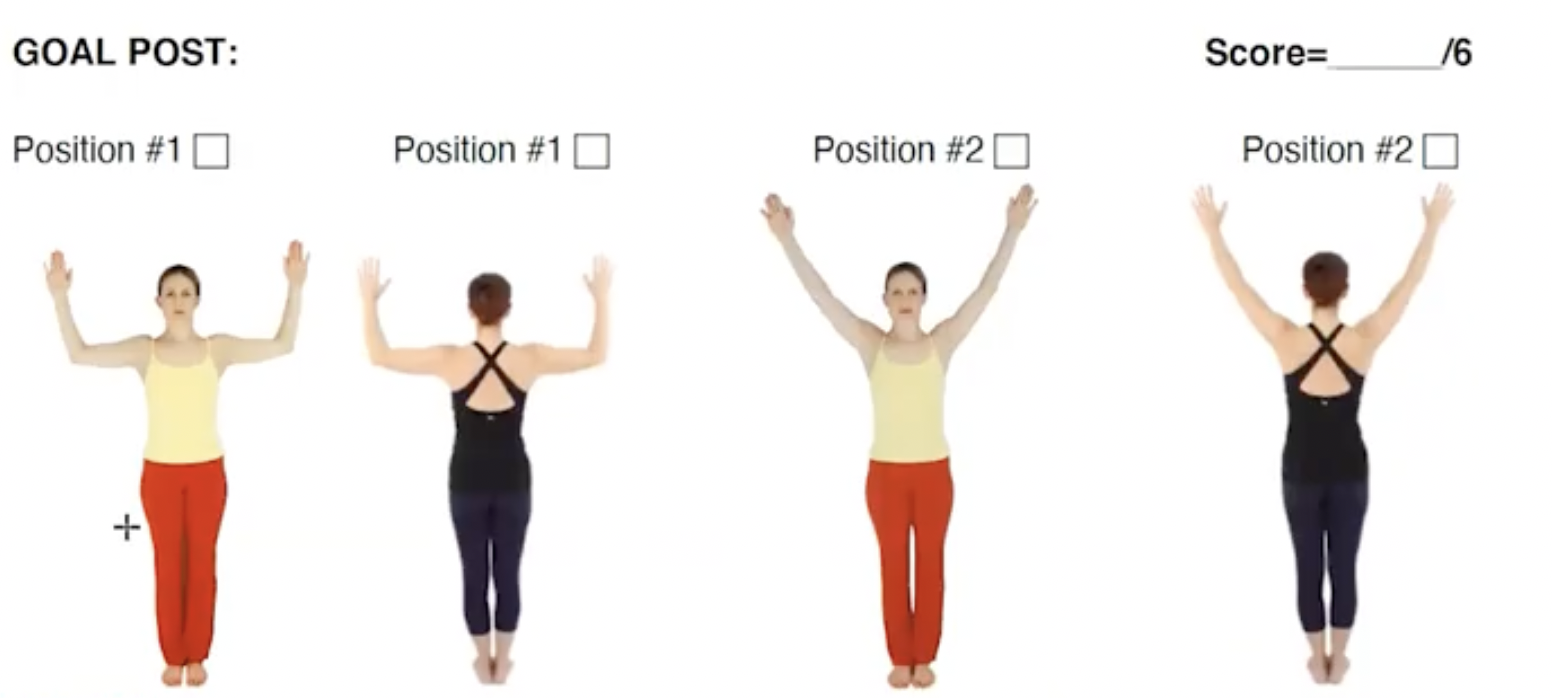
What information can we gather by watching someone perform the goal post?
When assessing the Goal-Post exercise, the client is asked to do three things:
Stand up against the wall with their head against the wall
Bring the arms to 90/90
Bring the arms into a high “V” position
Before cueing the exercise, the first thing to look for is axial alignment. Can the client position their head over their thorax and thorax over their pelvis while maintaining natural lumbar and cervical curves?
After looking at axial alignment, we look to see what is happening in the shoulder region?
What are some of the things required to be able to bring the arms into a 90/90 position and into a “V” overhead?
Shoulder Flexion
Shoulder Rotation
General Shoulder Mobility
Question:What else connects with shoulder mobility?
Answer: Thoracic mobility -This is one of the things to look for first when moving into the goal post as it directly impacts shoulder mobility. If the thoracic spine doesn’t move into extension, the following might be seen:
The head comes away from the wall
The shoulder girdle can’t slide down into its 90/90 position
The back may come away from the wall
Other tests and measures to use to confirm the possibility of a loss of thoracic mobility depend on how other aspects of the movement are functioning.
What can be ruled out?
Could it be a loss of scapular mobility?
Could it be a tight pectoral girdle or a loss of humeral rotation in the shoulder such as a rotator cuff injury?
During the assessment keep in mind, that it could be any of these things and then begin ruling them out.
Video of Brent teaching assessment using the goal-post exercise.
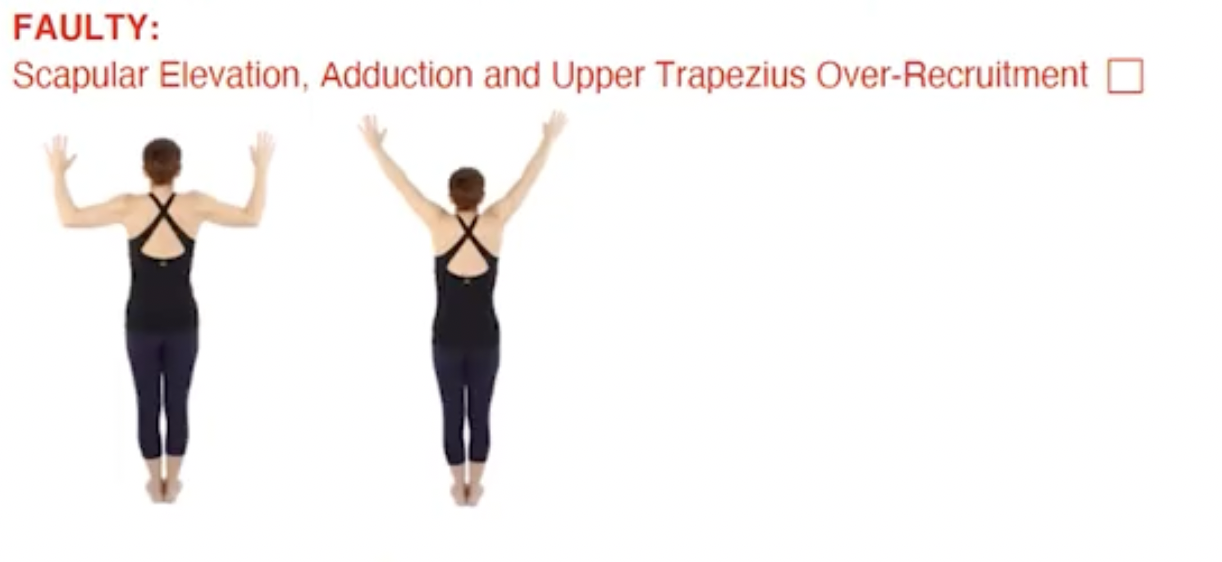
Faulty movement patterns that could be present:
The shoulders hiking up to perform the movement (bilaterally)
The pronation of the shoulders (very common)
Critical Reasoning: Is the client’s limitation in the thoracic spine or in the shoulder girdle? What other tests might we perform to distinguish between the two?
Asymmetries during Assessment:
When you see an asymmetry, you must seek to understand what the asymmetry is due to. You may see a client who can move one arm back nicely but not the other. If there is scoliosis or a spine deformity, the client might have an asymmetry where one shoulder is being rotated forward.
If there is no scoliosis or spine abnormality, then what is happening at the shoulder blade?
Is there a winging of the shoulder blade or poor organization of the shoulder blade?
What is happening at the glenohumeral joint?
How is it in relationship to the rest of the shoulder girdle?
Assessment Tip: Circle back to the client’s history.
Did they have an injury?
Is there any nerve pain? (A brachial plexus lesion could easily cause a limitation in bringing the arm up to 90/90.)
Critical Reasoning: Inquire about the client’s habitual patterns, as some of these daily patterns can create asymmetries, for example:
Someone who is always using the computer mouse with tension the right shoulder.
Someone who sleeps on one side causeing the shoulder to collapse forward.
The PT and medical world uses what’s called “upper limb tension testing”, one of which tests is to bring the arm up to 90/90 and then straighten it. A significant amount of people who have had brachial plexus lesions or a thoracic outlet syndrome lose the ability to bring one side up.
Assessment Tip: When an asymmetry is present in an assessment, remember to put a “red flag” on it. Asymmetry means there could have been an injury or something else going on that is challenging the movement.
Keep in mind – As we Assess we are always:
Ruling out
Asking questions
Seeking to understand: “What possibly might be causing this?”
Get the most out of your Assessment andEarn 24 NPCP CEU’s this Summer!
Join us for our upcoming immersion into Critical Reasoning and Assessment Skills:
I had osteoarthritis and my bones were wearing out from all of the movement that I did. Raising kids, being an early childhood educator, and my daily exercising, swimming, and walking, I have been very active. I think all of this movement, plus my genetics wore out my hip joints! When you are able to move, and then you realize “I’m just not moving” someone needs to have a look. My first experience doing Pilates was taking a couple of classes with my daughter at the Polestar Physical Therapy Center in Miami, Florida. We thought “let’s try something new, a new way to exercise”. Later I was invited to a Pilates teacher training at the center to participate as “a body” with student teachers who were practicing. They led me in Pilates and assessed my skills, and between my two hip replacements, they did a fantastic job! What I liked about Pilates is it’s all about me, it’s “me time”. Even when there are 5 other people in the room my instructor says “you can make it heavier, lighter, or try alternate positions”. I love that this helps me customize my movement and it keeps my joints lubricated.
My New Motto: “Good to Go”
Before my hip replacements, I was an event planner at an elementary school. I remember as my hips were getting worse thinking, “please don’t give me a job where I have to walk across campus to the other building”. After the first hip replacement, I was able to take long walks with my husband, bend, stoop, balance and move, and be with my grandson Zeb. I could take trips with my sister without worrying about pain. My motto became “good to go!” and I was thrilled to walk anywhere pain-free! For both of my hip replacements, I received physical therapy at the hospital. I loved moving with my PT and thought to myself “I bet she is a Polestar Pilates graduate” and not to my surprise she was. We did movement on the elliptical machine, walked on the treadmill, and presses and lifts on the equipment. Then I learned the clamshell, bridging with the ball, quadruped, and what I call the “donkey kick” – you push your leg up, up, up!
Pilates helps me keep everything moving!
Pilates helps me be with the people I love, other like-minded people at the studio, my husband, and my family. It helps me feel comfortable in my movement and helps me feel happy (it even helps in your romantic life) I Can Move! Pilates is really a total self-care practice, for well-being, mental health, emotional health, and of course physical health. My sense of well-being improves when I’m moving and I don’t feel like “the number 67” (my age). I feel younger in my body, mind, and heart. Pilates is “me time”, I get to give myself the love and care that dominoes to the other people I love and care about. Now I go to my neighborhood Pilates studio 2 or 3 times a week during the summer and fall.
I have fully recovered from two hip replacements, I enjoy providing childcare for my 18-month-old grandson Zeb. From picking him up and holding him, bending over, sitting on the floor with him, and playing in the tunnels. He even rides my back like a horse as I crawl around. I can enjoy bending over to change his diaper, walking him in the stroller, and playing with him at the park. We go to music class to play instruments, sing, and dance, and I love it all! I think for a senior person, especially, it really is all about moving. If you lead a sedentary life and are not active, not with people you won’t feel great. You just have to move! Pilates gives me that opportunity to gently and effectively move and enjoy so many things like fully participating with the ones I love.
Lyn Zuckerman is a retired early childhood educator living in Denver, Co.
Polestar Faculty Nichole Anderson, NCPT has had the pleasure of working with many clients with MS and has enjoyed the constant learning process it has provided.
“disease that involves an immune-mediated process in which an abnormal response of the body’s immune system is directed against the central nervous system (CNS) which includes the brain, spinal cord and optic nerves”.
In other words, MS involves a person’s immune system attacking their nerves. In our huge network of nerves, information has to travel quickly to allow us to act spontaneously. Many nerves are covered in myelin. This both insulates and accelerates the rate at which information travels in the nerve. When the immune system consistently attacks the myelin, it becomes damaged and forms scar tissue (sclerosis), which gives the disease its name. As the disease progresses, the nerve fiber itself can become damaged and destroyed.
What does this mean on a larger scale? When the myelin is scarred or the nerve fiber damaged or destroyed, a large number of nerve impulses from the brain and spinal cord are interrupted and/or distorted. All actions in the body and brain are triggered by some sort of nerve impulse which is why symptoms can vary from person to person.
Who Gets Multiple Sclerosis?
Without getting too deep into the epidemiology of MS, here are a few facts:
MS is a very difficult disease to diagnose. There are currently no single tests for MS. Because of this challenge, MS is often misdiagnosed or not diagnosed at all. Most epidemiological statistics on MS are estimates.
Most people are diagnosed between the ages of 20 and 50.
In general, MS is more common in areas further from the equator. There are many communities far from the equator that have little to no reported incidences of MS.
MS is at least 2-3 times more common in women than men.
Genetic factors seem to play a large part in determining who develops MS.
As with many diseases, MS is believed to be triggered by an environmental factor, as yet unidentified, in a person who is genetically predisposed to respond.
What Are The Common Symptoms?
Because of the variety of symptoms associated with MS, every client with MS will have different struggles in regard to movement. That being said, there are a few things that are very common in clients with MS:
Foot drop: This is where there is weakness in the muscles that dorsi-flex the ankle. When this progresses, walking can be dangerous as there is an increased fall risk.
Numbness: This is often one of the earliest and most common symptoms of MS. It can be numbness anywhere in the body, face, and extremities. It can cause the affected area to be disconnected and difficult to control. We will discuss later some ways to facilitate movement when certain body parts are numb.
Fatigue: In a movement class, this often means being unable to do high repetitions of movements, especially at a high load.
Weakness: This can occur from basic deconditioning of muscles that aren’t used due to damage to the nerves that stimulate them. Weakness can also occur when a client with MS has gotten overheated or fatigued.
Spasticity: This is when there is an involuntary muscle spasm that can cause prolonged rigidity in the limb that is spasming.
Considerations For Working With Clients With Multiple Sclerosis
Keep it cool!: A warm room can create a challenging movement experience for someone with MS and can even precipitate a flare-up.
Take frequent breaks: Even if your client feels like they can keep going, it is important to take frequent rests to avoid fatigue.
Spot, Spot, Spot!: While this is dependent on ability because MS frequently causes numbness, it is important to spot any moving apparatus that can slip out of a hand, off a foot, and onto your face
Suggestions For Building A Session
Warm up with hand and foot stimulation and movement. Depending on ability, I either do this for clients or have them do it to themselves. This can include:
toe pulling, tapping the bottoms of the feet with fingers
vigorous rubbing of the feet and ankles
interlacing fingers with toes and making circles
active movement of the ankle such as tracing the alphabet in the air with each foot.
Hand stimulation and movement: This is a great time to move an area that we don’t traditionally “exercise” in Pilates. I like to have people move through tight fists to hands stretching wide, followed by “piano fingers”. This can look like playing a fake piano slowly and quickly, getting some individual movement in each digit. After getting some movement, I give them some free time to self-massage their hands, rubbing them together vigorously. Another good activity can be kneading the palm of one hand with the other, and interlacing the fingers and squeezing.
Allow Transfers To Become A Part Of The Class
Depending on how far the disease has progressed, one of the most challenging parts of a class can be the transfer of one position to another. I like to discuss strategies for making these transitions. This could be gazing, moving from sitting to standing, maybe pausing somewhere in the middle of a transfer to do some movement there. It can also be supportive to allow time for clients to settle into the next position, allowing them to rest from the transition. This is also great because it is functional and allows clients to have strategies for getting out of sticky situations when they are going through their daily lives. I also like to help my clients explore their breath by spending time in each class breathing and working on the movement of the diaphragm and ribcage.
Work Safely On Balance
Use the equipment to your advantage! I often pull the tower bar through to the back and attach the safety strap. This creates a solid bar they can hold to practice heel raises or balancing on one leg. I also find the Core Align to be a great tool for working with clients with MS as it enables reciprocal leg movement with the support of a ladder to hold on to.
Support Distant Extremities :
Use velcro straps to connect feet to the footbar and hands to dowels if there is too much numbness in the feet or hands to hold on well.
Utilize Y-straps to secure both feet and hands when doing work with springs and pulleys.
Use therabands to hold thighs together for bridging, pelvic clock, and other exercises that require legs to be still. This is only necessary if the client is struggling to connect to their legs.
Use your tactile cues to bring awareness to less responsive areas. With your client’s permission, palpate areas that are not connecting well to help them find their feet, hands, legs, etc before going into a movement.
Keep In Mind That No Two Days Are Alike
What may have been strengths one day may be weaknesses other days. The temperature outside, activities of the day before, stress and other external influences can vastly affect the capabilities of clients with MS from day to day. It is always important to check in, and to allow for progress to be relative
Connect with Polestar Educator Nichole Anderson on social media @nicholemoves.
This article includes information from The National MS Society Nationalmssociety.org
What Is Intra-Abdominal Pressure And Why Does It Matter?
Intra-abdominal (IAP) pressure is defined as the steady-state pressure concealed within the abdominal cavity and resulting from the interaction between the abdominal wall and viscera; IAP oscillates according to respiratory phase and abdominal wall resistance.
How do we educate people who have lost the capacity to appropriately use intra-abdominal pressure? Think about the following statement:The appropriate amount of stiffness for the anticipated activity. What does this best describe? Stability? Core Control? Powerhouse? All of these things?
The answer is all of them. Whether we are talking about stability, the powerhouse, or core control, we should be talking about the same concept. That is, does someone have the right amount of support for the anticipated load or activity? I intentionally use the word anticipated. The brain is using information from past experiences to determine the best approach. This enables us without thinking to know how much stiffness to create in preparation for picking up a jug of milk versus a bag of dried leaves for example.
Joseph Pilates implied that the powerhouse is where things start. What kind of tools do we as movement practitioners have to facilitate the appropriate amount of stiffness for the anticipated load? When asked how they would rank the greatest influencers of intra-abdominal pressure, our #PilatesHour webinar attendees answered as follows:
A lot of people think it is about muscle control or abdominal strength. This is not the case. When we talk about the abdominal wall and intra-abdominal pressure with our clients, we often confuse them. This is because intra-abdominal pressure involves much more than just the abdominal wall. Intra-abdominal pressure is the stiffness inside the trunk, particularly in between the chest and the pelvic floor. It is this stiffness that is necessary to control the amount of movement based on the load.
The Power Of Breath
Breath is a powerful influencer of intra-abdominal pressure. The diaphragm is in fact one of the primary muscles and controllers of intra-abdominal pressure. Some people do not utilize the breath or the diaphragm efficiently or as part of dynamic control. This provides a terrific opportunity for Pilates instructors to affect IAP simply through training efficient and supportive breath patterns.
The appropriate amount of stiffness is going to be determined by the activity and facilitated by proper alignment. For example, holding your breath in and of itself will create stiffness, but does it create the appropriate amount of stiffness? Is this a stiffness or support that can be maintained for a period of time? Proper alignment and practice lead to efficient and successful movement that seldom has to do with core strength.
Most of our bodies are given the appropriate amount of strength to be able to handle the movements we choose to participate in. That does not mean that tomorrow, with my body in its current condition, I can go out and perform a 400-pound deadlift if I chose to. I am not conditioned for this activity, nor do I have a need to lift 400 pounds.
However, if I were training to perform that specific loaded movement, my body would naturally start gaining strength by steadily increasing the deadlift weight. Tissue adaptation would happen, meaning that my abdominal wall, my back muscles, and my pelvic floor would all start to change based on the demand that I would be making on those tissues.
This leads to the question, How much control, mobility, or stiffness is necessary to accomplish the task at hand?
Let’s say the box in this photo weighs 40 pounds. What parts of his body must recruit and create stiffness to keep him from falling? What if the box were 100 pounds, vs 15 pounds. How would that change the situation?
When we look at the dynamic movement of kicking a ball, what are they doing and what muscles must be turned on for the person in the photo to be able to kick the ball? Which fascial trains or slings are being activated or tensioned to be able to have the appropriate amount of control of the trunk so that their leg and body can accelerate the foot through space and kick the ball down the field?
How can we support clients in improving the efficiency of their intra-abdominal pressure?
Help them find their optimal alignment
Help them find efficient breath patterns within their optimal alignment
Progressively load them, working always within ranges where they can maintain the above
Work through the above points to help them perform the activities in which they want to participate
With this basic introduction to intra-abdominal pressure, we see that it is more about alignment, breath, and load than focused abdominal work. I encourage you to try facilitating the above points with your clients and see how their quality of movement and integration with activity improve.
Brent Anderson, PhD, PT, OCS, NCPT is the President and Founder of Polestar Pilates International. Brent is a licensed physical therapist and orthopedic certified specialist with more than 22 years of experience. Based on his extensive background in rehabilitation and movement science, Brent elaborates on Joseph Pilates’ mind-body work through the Polestar curriculum by developing tools for critical reasoning and applying supportive scientific research. He also infuses the integral role of psychology and energy systems on motor control and motor learning.
There are many ways in which we can guide our clients through movement. We can use a vast variety of verbal and tactile cues to help them change their movement habits and master increasingly complex challenges.
How often do clients tell us that unless we put our hands on them to guide them in the right direction, they are unable to replicate the experience?
And how often do they say, after a complex piece of work, that there is so much to think about? That they have to concentrate so very hard to coordinate everything? While feedback like that is common we should consider carefully what the client is really telling us.
As a Somatic Practitioner and a Pilates teacher, my goal almost always is to help people become more aware of sensations. Sensations provide vital information about our physical and mental well-being. Being present in our body and in tune with its sensations is not just an essential part of healthy movement practice. It also adds to our overall resilience and life vitality. It alerts us of physical and emotional strain, so we can take action before problems turn chronic. It allows us to make better decisions. It makes us better at resourcing ourselves with what helps us maneuver through tough times so we are less prone to trauma.
“There Is So Much To Think About In Pilates!”
One day one of my clients sighed: “there is so much to think about in Pilates!”. I had to pause and try to understand what they were really saying. The way in which the client sighed their words told me that the experience had somewhat overwhelmed them. When we are overwhelmed it is much harder for us to be and remain in our bodies. This is especially true if we are not used to it and trying to make sense of something new at the same time. The fact that they had to “think” a lot while moving told me they may have not been “in their body” at all during the past 20 minutes of our one-on-one Pilates session.
Our conscious thoughts happen in our prefrontal cortex, also known as the thinking brain. This is the youngest part of our brain and also where our modern society requires us to be focused most of the time. From a young age, we are expected to understand rules, keep to a schedule, and use logical reasoning to navigate through life. The older parts of our brain, the limbicand reptilian brain, concerned with emotion, instinct, and physical sensation, become subdued and controlled by the prefrontal cortex. If we are upset we try to pull ourselves together. If we feel threatened by something that we can not logically explain, we feel ashamed and try to hide it. If we have pain, we numb it with painkillers.
Pilates, as an embodiment practice, should help us reconnect with our instincts and physical sensations, yet all my client experienced was their thinking brain coordinating their movements. I had thoroughly failed at providing my client with the basics of an embodied movement practice.
Kristen Loeer
Firstly I had to look at my own insecurities that had led me to overwhelm my client. My desire was to give them all the wonderful cues, visualizations, and information that I knew. I had been driven by my thinking brain, which would tell me that unless I did everything I possibly could, I was being lazy, holding back, and not giving my client enough.
What might this have been like if I were more in tune with the oldest, most instinctive part of my brain, my reptilian brain? Perhaps I would have been less distracted by my beliefs about my worth as a Pilates teacher. I may have picked up on the silent and physical clues that would have told me that my client was overwhelmed. That they were trying to figure it all out in their head, rather than communicating with their body. The first steps were for me to realize that I had more embodiment work to do myself.
This experience also made me more aware of our “cueing tool kit” and how we use it. Could it be that the way we cue our clients favors addressing their thinking brain, rather than promoting embodiment?
Dr. Peter Levine’s SIBAM Model
Dr. Peter Levine introduced the SIBAM model representing all of the elements of human experience; S – Sensation, I – Image, B – Behaviour, A – Affect, and M – Meaning.
When we have a traumatic experience, one or more elements can get split off from our awareness. For example, we might be unable to remember what we did during the traumatic event (behavior). We may feel numb when we talk about what happened (affect). Ideally, we have a fairly balanced awareness of all the elements in order to best integrate the experience moving forward in life.
If we apply the SIBAM model to the experience of practicing a Pilates exercise, such as semicircle on the reformer, it could look like this:
Sensation: The physical sensation of feeling the pressure of the foot bar under our feet. Feeling a sense of expansion or containment, as we reach into the shoulder rests and foot bar. The heat or tension generated by the stress our body is experiencing during this exercise. Is there intensity? Does intensity turn into tension and struggle? Is there pain? Do we feel connected?
Image: The visualization of my spine riding a wave. The image of myself as a dolphin-like creature. I can imagine my sitting bones moving apart and closer together throughout the movement. Maybe I am literally seeing myself in the studio mirror.
Behavior: The movement that is semicircle is essentially the behavior, but also the strategy I am using to move through this exercise is part of the behavior. In short: “what am I doing?” and “how am I doing it?”
Affect: Any experience has an emotional component. Perhaps I feel joy at experiencing this fun, flowing exercise. Maybe there is a slight sense of unease, irritation, or fear attached to the movement.
Meaning: The meaning we give the movement is a semicircle. As we say the word semicircle we already have a meaning attached to the movement. Perhaps the meaning is “integrated, pleasurable exercise that helps my spine gain mobility.” Or maybe I have a belief about this exercise putting me at risk of hurting myself.
I do want my client to be aware of all the elements of their movement experience, but as mentioned earlier, we tend to learn from an early age to rely heavily on our meaning and belief-making brain. We don’t tend to be very in tune with our more subtle physical sensations.
For example, when you are happy, how do you know you are happy? The emotion you are naming as happy always comes with physical sensations. But what are those sensations, can you name them?
You may find that it is not all that easy, because these sensations can be rather subconscious. However, if they were not present you would not be able to identify what you are feeling as happiness. Becoming more aware of the sensations in our bodies is what helps us become embodied. If I can feel the mat underneath me if I am confident about where I am in space. If I can detect the first level of bracing in my muscles and make an instinctive change that allows me to relax. This means I am in my body and truly communicating and working with it.
When I explain to my client that we are going to do semicircle on the reformer and give them the general instruction of what goes where I am setting up the behavior coupled with meaning. We are doing semicircle and this is how the movement goes.
As they start moving I might notice aspects of their strategy that do not look so efficient. That is when I might offer a cue: “dive your tail through the water like a dolphin,” or “send your sitting bones to the back of your knees.” In terms of SIBAM, I am still cueing behavior with the help of an image.
It is only when I draw my client’s attention to their proprioception (awareness of themselves in space) and even more importantly their interoception (awareness of internal sensation) that I begin helping my client embody semicircle. I may also offer tactile cues. In fact, this can initially be very helpful for those who struggle with feeling their body. It is much easier to recognize the sensation of someone’s hand on me than the sensation that comes with happiness. Tactile cueing can be a great starting point to help clients become more embodied.
Ultimately tactile cues are only helpful if the client can be aware of the sensation of the touch, in addition to the sensation of the change that the tactile cue has caused in their body’s movement. Only then can they apply the changes internally that help them move better. Otherwise, the client will not actually integrate the changes we are making and simply go back to their old patterns.
Awareness Of Affect In Pilates
Another element of SIBAM we hardly ever promote awareness of in Pilates is the affect. Have you ever acknowledged a client’s excitement after managing parakeet for the first time. Do you respect a client’s fear of a suggested exercise and find a compromise? We do not tend to dedicate much time to engaging with emotional responses. Of course, that may be for good reason. There is a fine line between encouraging someone to feel their pride and confidence at achieving parakeet, and the boundaries of the scope of practice as a Pilates teacher when it comes to managing more challenging or negative emotions that might be attached to a movement.
Promoting embodiment and the awareness of one’s body in movement is certainly an essential part of teaching Pilates.
Promoting true embodiment in our clients means having to assume less and ask more questions. I can make my client aware of sensations that I can assume they are able to feel. I can say: “feel the contact that you are making with the reformer”. “Feel your relationship with gravity changing,” or “allow your head to be heavy.” This is where our ability to assume things ends. Sensations are highly subjective and we can not know what our clients are sensing on a more subtle level. W can only be observant and ask them about the sensations they are experiencing. This also makes our clients feel seen, communicating more actively with me and taking ownership of their session.
I can ask a relatively directive question about my client’s sensations, like: “can you feel your jaw releasing?” or “can you feel your connection through your right arm into your center change as you hold the bar differently?” The client has to feel into these specific areas in order to answer the question. I could also ask more open questions to allow the client to expand their awareness and gain new insights into themselves in the movement. I could ask: “as you are gaining more flow, what changes are you aware of in your body?” or “what was happening in your body just then, before you lost stability?”
The Client is the Expert of Themself
Ultimately it is my goal always to make my client the expert of themselves. I am not there to tell them what they should be feeling or how they should be moving. My goal is to help them get to know their unique self in movement. I am there to help them engage with their body to learn how they can improve their movement ability. I respect that we are all different and that our experiences are also different. While I may help them orient and navigate, ultimately their experience will be different than mine and only they can experience themselves moving.
When experimenting with more sensory or somatic cueing, it is also important to be mindful of our pace, giving too much information, and asking too many questions. Sensing into what the body has to say while we are moving requires us to slow down a lot.
Many clients will struggle to access physical sensations, particularly if their brain is busy with figuring out what (behavior) they are doing, or why (meaning). If I am engaging with semicircle for the first time, I easily resort to connecting with the part of me that I am most used to consulting. My thinking brain goes into overdrive trying to figure out where I am in space. How do I engage with this spring tension? What is this movement or choreography? My felt sense would be a very authentic, wise, and safe advisor in this.
It is easy for teachers to buy into this struggle by wanting to offer more clarity with more cues serving meaning, behavior, and image. This may get us some success in terms of our client being able to navigate through the movement. Telling someone what to do is quicker and easier than asking the client to be comfortable in confusion and taking the time to help them sense into their body and figure out what feels true to them. However, if we allow the client to rely on their thinking brain too much to master the exercise, we will see them putting their body through a potentially risky movement, with no or very little awareness of themselves and no deep learning that could enable authentic change or growth.
If we provide the right environment and remain mindful of our pace, sensory cueing will make an incredible difference to our client’s experience. If we can cue and support our client in a way that enables them to be embodied from the beginning to the end of an exercise, we will see a client who is moving confidently and well, fully aware of what is happening in their body, and fully in control throughout, having a calm and enriching experience.
All we need to do is be in our body ourselves, aware of our own sensations, as they will guide us to promote the same in our clients, without pushing or overwhelming them.
Roxana’s extensive training in Rehabilitative Pilates and the John F. Barnes Approach to Myofascial Release gives her patients a unique healing experience. She is trained in Pilates Rehabilitation from Polestar Pilates, as well as certified by the Pilates Method Alliance (PMA). For several years, she taught at Polestar Pilates Studio in South Miami, FL and she is an active educator for Polestar education. As a practitioner, Roxana goes above and beyond to educate, heal, and guide her patients and clients to attain and surpass their goals so that they can live a life of maximum potential, free from pain and dysfunction.
In your own words – describe “the Spirit of Polestar”
RML: It is the spirit of living our best life and sharing it with those around us. The Polestar spirit connects us all as one, all over the world as movement specialists and as novice observers. It is an openness to learn from every experience with an open heart and mind in order to continue growing in the journey of self-discovery and improvement.
What Three Words come to mind when you think of “Polestar Pilates”?
Inclusive
Intelligent
Empowering
What do you love about teaching Pilates?
RML: I truly love to teach, as I feel a sense of great satisfaction when sharing my knowledge with others. I also learn so much from teaching. There are many times that I have unexpected “aha” moments and continue to grow with each experience. I approach life as an apprentice and I learned from an early age that there is always more to learn. This year has taught me patience and resilience. In 2019, my family and I moved from Miami to Palm Beach and along with my business partner, we opened our first Pilates studio and Physical Therapy Clinic in December. Our grand opening was on February 27, 2020, the week of state closures due to Covid-19. It has been a challenging, but tremendously growing experience. I am very grateful to be part of the Polestar community because in this trying time, it has helped me stay focused and grounded. I was trained by Polestar and happy to become an educator after 6 years as a mentor.
What are your current Inspirations?
RML: I am inspired by people like Mother Teresa who dedicated their lives to helping others in need. I’m also inspired by my grandmother. She was a self-proclaimed nurse. I have vivid memories of her spending her time visiting the local monastery in Cuba and aiding the sick. These women were humble, selfless, and sacrificial.
Why Pilates? How did you find the practice?
RML: As a teenager, I enjoyed fitness and dance. I was trained in modern dance and was a cheerleader. I had an inclination to sports rehabilitation early on in my career and one of my good friends, Michele Gust, insisted I learn Pilates. I took Pilates fitness classes in my local gym and started adapting some of the exercises as treatment for my back patients. The patients loved it and I had very positive results.
Why Polestar Pilates? How did you come to join the Polestar Community?
RML: Michele continued to insist that I should be formally trained through Polestar. It took me 10 yrs to finally register and complete the Polestar Education Program.
What do you hope to convey in your teaching?
RML: In my teaching, I hope to convey freedom of expression, understanding of purposeful movement and how movement impacts the body.
What is your favorite Quote?
“Be kind whenever possible. It is always possible.”
Dalai Lama
I try to be kind to everyone I come across because life is full of challenges and if you can bring some light into someone’s day, it can influence their mood.
What is your Favorite Apparatus or favorite way to move?
RML: I love the Trapeze Table because it allows much freedom of movement. You can hang upside down, twist and turn, and it feels like a playground.
We use technologies like cookies to store and/or access device information. We do this to improve browsing experience and to show (non-) personalized ads. Consenting to these technologies will allow us to process data such as browsing behavior or unique IDs on this site. Not consenting or withdrawing consent, may adversely affect certain features and functions.
Functional
Always active
The technical storage or access is strictly necessary for the legitimate purpose of enabling the use of a specific service explicitly requested by the subscriber or user, or for the sole purpose of carrying out the transmission of a communication over an electronic communications network.
Preferences
The technical storage or access is necessary for the legitimate purpose of storing preferences that are not requested by the subscriber or user.
Statistics
The technical storage or access that is used exclusively for statistical purposes.The technical storage or access that is used exclusively for anonymous statistical purposes. Without a subpoena, voluntary compliance on the part of your Internet Service Provider, or additional records from a third party, information stored or retrieved for this purpose alone cannot usually be used to identify you.
Marketing
The technical storage or access is required to create user profiles to send advertising, or to track the user on a website or across several websites for similar marketing purposes.