What information can we gather by watching someone perform the goal post?
When assessing the Goal-Post exercise, the client is asked to do three things:
- Stand up against the wall with their head against the wall
- Bring the arms to 90/90
- Bring the arms into a high “V” position
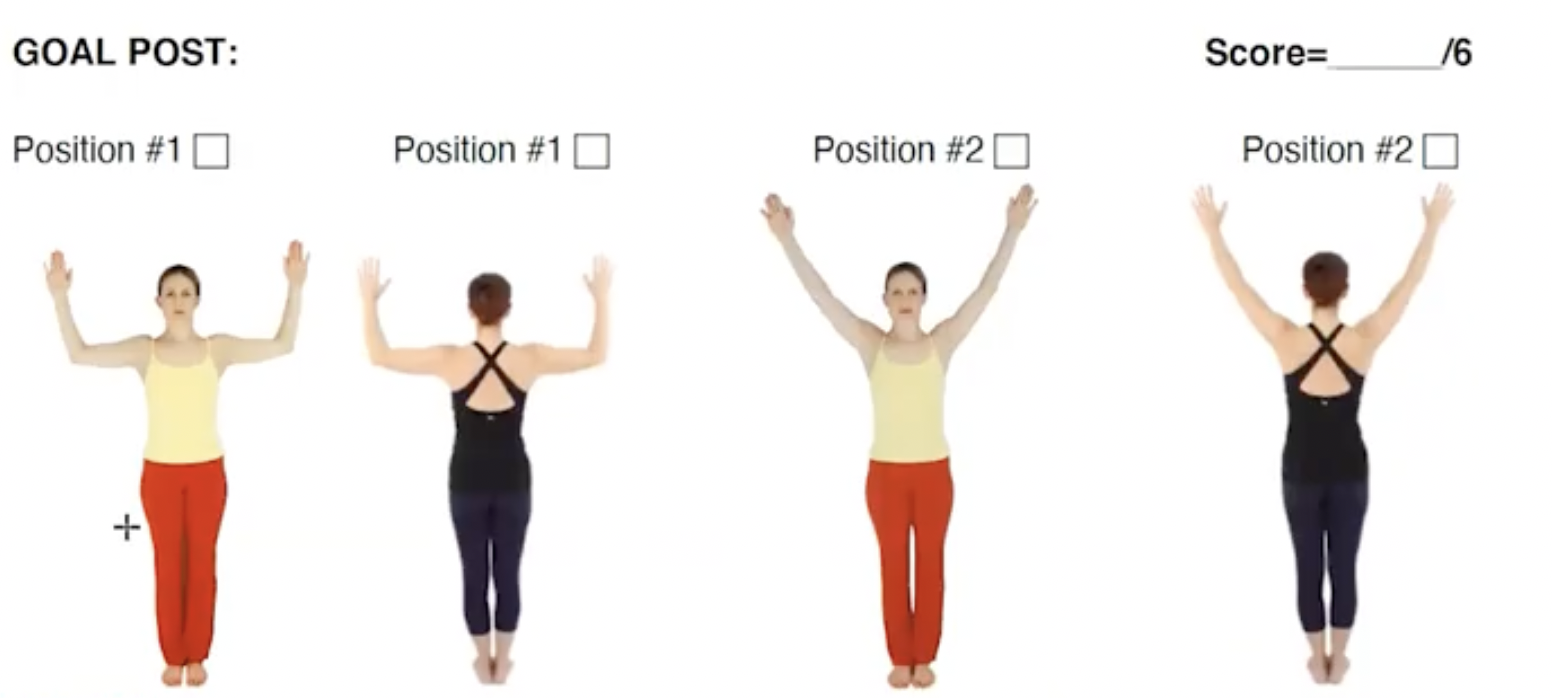
Before cueing the exercise, the first thing to look for is axial alignment. Can the client position their head over their thorax and thorax over their pelvis while maintaining natural lumbar and cervical curves?
After looking at axial alignment, we look to see what is happening in the shoulder region?
What are some of the things required to be able to bring the arms into a 90/90 position and into a “V” overhead?
- Shoulder Flexion
- Shoulder Rotation
- General Shoulder Mobility
Question: What else connects with shoulder mobility?
Answer: Thoracic mobility -This is one of the things to look for first when moving into the goal post as it directly impacts shoulder mobility. If the thoracic spine doesn’t move into extension, the following might be seen:
- The head comes away from the wall
- The shoulder girdle can’t slide down into its 90/90 position
- The back may come away from the wall
Other tests and measures to use to confirm the possibility of a loss of thoracic mobility depend on how other aspects of the movement are functioning.
- What can be ruled out?
- Could it be a loss of scapular mobility?
- Could it be a tight pectoral girdle or a loss of humeral rotation in the shoulder such as a rotator cuff injury?
During the assessment keep in mind, that it could be any of these things and then begin ruling them out.
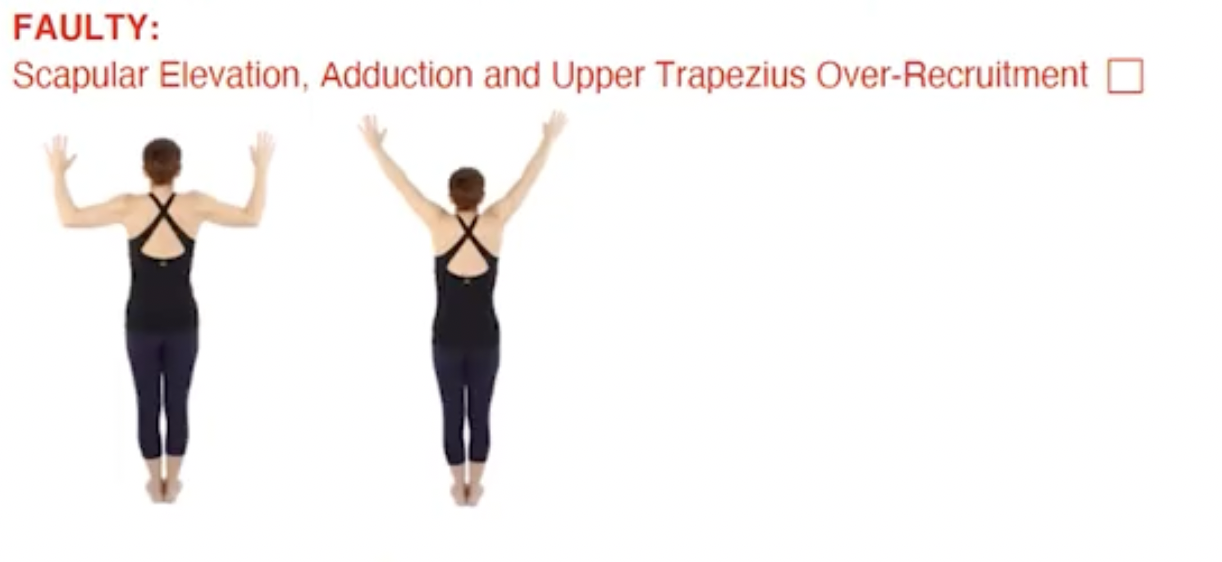
Faulty movement patterns that could be present:
- The shoulders hiking up to perform the movement (bilaterally)
- The pronation of the shoulders (very common)
Critical Reasoning: Is the client’s limitation in the thoracic spine or in the shoulder girdle? What other tests might we perform to distinguish between the two?
Asymmetries during Assessment:
When you see an asymmetry, you must seek to understand what the asymmetry is due to. You may see a client who can move one arm back nicely but not the other. If there is scoliosis or a spine deformity, the client might have an asymmetry where one shoulder is being rotated forward.
- If there is no scoliosis or spine abnormality, then what is happening at the shoulder blade?
- Is there a winging of the shoulder blade or poor organization of the shoulder blade?
- What is happening at the glenohumeral joint?
- How is it in relationship to the rest of the shoulder girdle?
Assessment Tip: Circle back to the client’s history.
- Did they have an injury?
- Is there any nerve pain? (A brachial plexus lesion could easily cause a limitation in bringing the arm up to 90/90.)
Critical Reasoning: Inquire about the client’s habitual patterns, as some of these daily patterns can create asymmetries, for example:
- Someone who is always using the computer mouse with tension the right shoulder.
- Someone who sleeps on one side causeing the shoulder to collapse forward.
The PT and medical world uses what’s called “upper limb tension testing”, one of which tests is to bring the arm up to 90/90 and then straighten it. A significant amount of people who have had brachial plexus lesions or a thoracic outlet syndrome lose the ability to bring one side up.
Assessment Tip: When an asymmetry is present in an assessment, remember to put a “red flag” on it. Asymmetry means there could have been an injury or something else going on that is challenging the movement.
Keep in mind – As we Assess we are always:
- Ruling out
- Asking questions
- Seeking to understand: “What possibly might be causing this?”
Get the most out of your Assessment and Earn 24 NPCP CEU’s this Summer!
Join us for our upcoming immersion into Critical Reasoning and Assessment Skills:
Critical Reasoning for Rehabilitation and Post Rehabilitation, held this June in Siler City, NC with Polestar Founder Brent Anderson.




 I will be brief since this is a whole course in itself! We know that Idiopathic (no known cause) Scoliosis (IS) is a 3 dimensional spinal disorder that begins with anterior vertebral wedging due to RASO (relative anterior spinal overgrowth) during bone development. We also know that the rotational component of scoliosis exists as
both inter-vertebral torsion (rotation of one vertebra relative to another) and intravertebral torsion (an internal rotational distortion within each vertebra), most notably at the apical vertebra (the vertebra most deviated laterally from the vertical axis that passes through the sacrum).1
This distortion contributes to less joint motion at the apex of the curve and more at the transition points of the curve.
We see this to a greater degree in adults and to a lesser degree in adolescents who have a more flexible curve before bone maturity. This is apparent in a supine lateral flexion X-ray that assesses curve flexibility.
I will be brief since this is a whole course in itself! We know that Idiopathic (no known cause) Scoliosis (IS) is a 3 dimensional spinal disorder that begins with anterior vertebral wedging due to RASO (relative anterior spinal overgrowth) during bone development. We also know that the rotational component of scoliosis exists as
both inter-vertebral torsion (rotation of one vertebra relative to another) and intravertebral torsion (an internal rotational distortion within each vertebra), most notably at the apical vertebra (the vertebra most deviated laterally from the vertical axis that passes through the sacrum).1
This distortion contributes to less joint motion at the apex of the curve and more at the transition points of the curve.
We see this to a greater degree in adults and to a lesser degree in adolescents who have a more flexible curve before bone maturity. This is apparent in a supine lateral flexion X-ray that assesses curve flexibility.
 Better posture can be achieved by emphasizing the most fundamental principles of all intelligent movement disciplines: axial elongation and breathing. Scoliosis curve concavities are constantly under compression by gravity. Axial elongation encourages a natural re-alignment of the spine by using neuromuscular activity to reduce multi-plane compression and collapse of the concave side of the scoliosis curves.
Once the concavities (which include the ribs) are expanded, then breath can be used to further open the collapse through:
Better posture can be achieved by emphasizing the most fundamental principles of all intelligent movement disciplines: axial elongation and breathing. Scoliosis curve concavities are constantly under compression by gravity. Axial elongation encourages a natural re-alignment of the spine by using neuromuscular activity to reduce multi-plane compression and collapse of the concave side of the scoliosis curves.
Once the concavities (which include the ribs) are expanded, then breath can be used to further open the collapse through:
 A research article was published in 2014 claiming that scoliosis curves can be reduced by doing side planks on the convex side of the curve, and was sensationalized in a WSJ article.2 But the research had many flaws3 and while interesting, it cannot make that claim. Muscular activity on both the concave and convex side of a scoliosis curve is inefficient and exercises that address each side are optimal for IS, including the Side Plank. Consider benefits of the Side Plank based on curve type:
A research article was published in 2014 claiming that scoliosis curves can be reduced by doing side planks on the convex side of the curve, and was sensationalized in a WSJ article.2 But the research had many flaws3 and while interesting, it cannot make that claim. Muscular activity on both the concave and convex side of a scoliosis curve is inefficient and exercises that address each side are optimal for IS, including the Side Plank. Consider benefits of the Side Plank based on curve type:
 Life takes us out of neutral spine…shouldn’t we train our scoliosis clients how to move their spine effectively out of neutral? The answer is of course yes…. but which movements and how much? This depends on your assessment of the client: Are they in pain? How much movement does the apex of each curve have? What is the curve type? What other muscle imbalances or injuries exist? What are their goals? Considering that the scoliosis spine tends to move more at the transition points and less at the apices, we may want to limit end range movements and emphasize elongation in postural shapes that minimize compression of the curve concavities. This will be more difficult for those with a double curve. So it is important to make critical decisions with your client based on your evaluation and their goals.
Life takes us out of neutral spine…shouldn’t we train our scoliosis clients how to move their spine effectively out of neutral? The answer is of course yes…. but which movements and how much? This depends on your assessment of the client: Are they in pain? How much movement does the apex of each curve have? What is the curve type? What other muscle imbalances or injuries exist? What are their goals? Considering that the scoliosis spine tends to move more at the transition points and less at the apices, we may want to limit end range movements and emphasize elongation in postural shapes that minimize compression of the curve concavities. This will be more difficult for those with a double curve. So it is important to make critical decisions with your client based on your evaluation and their goals.